









Addressing Parafunction with QuickSplint®
Destruction of the dentition from grinding and clenching is a significant problem for patients and dentists alike. Often the amount of damage will necessitate complex restorative dentistry to restore the teeth. Dentistry’s preventative approach should be early recognition of potential parafunction and trial use of protection during sleep as early as possible. I have found QuickSplint® to be a convenient and easy anterior bite plane design that can be applied on a trial basis to patients almost universally.

Appliance therapy is a routine part of my practice. There are many diagnostic and therapeutic advantages to incorporating initial, short-term appliance therapy into a practice for many uses. As strongly as I feel about the clinical side of appliance therapy, without question the most important thing I use a transitional appliance for is behavioral. I have yet to find a tool that is as effective in increasing patient awareness and ownership as transitional appliance therapy using QuickSplint®.
The first step of the process is to invite the patient into transitional appliance therapy and develop an interest in what QuickSplint® can do for them. Patients come in with or without symptoms. In my experience, patients who present with symptoms (be they severe pain, chronic headaches or broken teeth) already have an interest in finding out how to get better or prevent future problems. With this said, I still like to create a connection between what the patient is experiencing and appliance therapy.
I have a large patient population that has no symptoms but I see signs that concern me and make me believe an appliance may be in their best interest. Again, the goal is to help them make this connection and build understanding. I long ago stopped telling patients that they grind their teeth. What I do share with the patient is what I see, including the physical evidence in their mouth of missing tooth structure that doesn’t seem appropriate for their age. I also share with them my concern about what this could mean for their dental health moving forward. We have an opportunity to learn what the cause might be and then we can discuss ways to protect and preserve their teeth; i.e. an appliance.
Once patients are wearing a QuickSplint®, we now have a device that is an incredible learning tool for everyone. Our role is not only to interpret what the appliance teaches us about the occlusion, joints and muscles but to create an opportunity for the patient to learn along with us. This learning is a balance between inviting the patient to be observant, listening to their experiences and conclusions and sharing appropriate information about the science behind appliance therapy.
The Anterior Bite Plane appliance, known by many names, is a highly effective and highly versatile design. QuickSplint® is a pre-formed shell that allows fabrication of a temporary anterior only appliance that is quick, efficient and cost-effective. The physiologic response from a QuickSplint® is the same as other anterior-only appliances that can be custom made. The ease and accuracy allows the use of QuickSplint® in the office for acute symptoms and as a patient education tool that creates ownership of their parafunctional activities and the relationship to their symptoms. Used clinically, you can overlay its use to your differential diagnosis of joints and muscles and have high predictability when using QuickSplint® therapeutically or diagnostically. This data creates a smooth transition into a custom fabrication of an occlusal appliance.
QuickSplint® is a fabulous tool in moving patients on to an occlusal appliance. The design is trim to the anterior teeth and comfortable to wear. A roadblock to appliance therapy can be the patient’s disbelief and lack of understanding that they parafunction and rub their teeth together. Previously I used a jig to help patients experience this relationship however it was not as suitable for overnight wear, what the cause might be and then we can discuss waysto protect and preserve their teeth, i.e. an appliance.
Differential Diagnosis
Addressing parafunction begins with a joint, muscle and dentition exam. This information allows us to formulate a differential diagnosis and understanding of the present condition. With this information we can utilize the proper design to alleviate symptoms, narrow our differential and assist the patient in adaptation. We want to utilize our joint exam to determine if there is inflammation present and to get an idea of the anatomic relationship between the disc and the head of the condyle in both rotation and translation. Definitive diagnosis of disc position requires joint imaging, but our clinical exam and a thorough patient history can give us enough information to make a preliminary appliance choice.
The ease of the QuickSplint® design and delivery makes this type of trial treatment ideal. Even for an inflamed acute joint problem QuickSplint® is a viable treatment preferable to no treatment on the first office visit. If the patient worsens, they simply stop use.
Experience has shown anterior bite plane appliances like QuickSplint® work best for patients with muscle-based signs and symptoms and healthy joints. These patients often present to us with complaints of headaches, muscle tension or fatigue during normal chewing. Often these patients may have an underlying pattern of grinding or clenching that is a contributing factor. By using an anterior-only appliance we can efficiently and effectively release muscles and relieve symptoms. Often these patients feel better within a few hours of appliance therapy.
Anterior bite plane appliances can be a great resource for patients with joint inflammation and a normal disc condyle relationship. Patients with disc displacements may benefit from an anterior bite plane appliance or the situation can be worsened. This depends on the nature and extent of the disc displacement, and the impact on muscle release the patient has without posterior tooth contact. By convention many practitioners simply do not use them for patients with any disc displacements. With an understanding of the disc displacement (medial versus lateral, reducing or nonreducing), the patient’s response to loading, and the additive presence of muscle involvement many practitioners find anterior-only appliances to be helpful. When prescribing an anterior- only appliance for patients with disc displacements careful monitoring for improvement or worsening of symptoms is a critical component of therapy.
All appliance designs can result in three possible outcomes: no change, the patient improving or the patient getting worse. Every one of these outcomes is important diagnostic information. We hope all of our appliances are therapeutic and the patient’s signs and symptoms are alleviated. Remember appliances are always diagnostic and often therapeutic as well. If the patient experiences no change, worsens or develops new signs and symptoms they didn’t present with, go back and re-evaluate your differential diagnosis. This re-evaluation may result in the recommendation to change appliance design.
Another roadblock to initiating appliance therapy has been the time (and associated cost) to make a custom temporary appliance. QuickSplint® is easy to make in minutes and the reline of the QuickSplint® tray, accomplished with a VPS of heavy viscosity, is rigid enough to eliminate concern over retention, but flexible enough not to produce orthodontic force on the covered teeth. Lastly, the device will last for several weeks allowing the patient to experience the positive experiences of less muscle tension, fewer headaches and better sleep, and the patient can see marks on the occluding surface of the plastic so they have physical evidence of the damage they do with their teeth.
Other Uses
Another great use of QuickSplint® is to allow the accurate recording of centric relation. Diagnostic models are best mounted in centric relation, so we can understand the difference between this position and intercuspal position, and plan where we will treat the patient based on their clinical findings. Muscle tension, tenderness or contraction can be a limiting factor in gathering accurate bite records. The use of an anterior-only appliance at night for 7-14 days is an easyway to release the muscles prior to taking bite records. QuickSplint® can be left in to aid in the process of acquiring a centric relation bite record with silicone.
Patients with muscle tightness or tension will commonly present with a limited range of motion. For some patients this can affect their quality of life and limit the foods they feel able to eat. Other patients aren’t aware of this issue until they have a need for dental work. The limit in their range of motion can make it difficult on both the patient and the dentist. Fabrication of a QuickSplint® and having the patient wear it for pre and post procedure use can dramatically increase their ability to open, aid in the successful completion of the process, and reduce post-operative discomfort.
Guidelines for Use
I instruct patients to brush and floss their teeth and then brush the QuickSplint® before putting it in. They reverse this process in the morning when they take the appliance out. Patients are asked to slowly close after taking the appliance out in the morning and pay attention to where their teeth touch. This will be a different bite than what they are normally accustomed to. They are also instructed to pay attention to how long it takes before they can touch their teeth together and find “their” bite. If this time begins to lengthen past 30-45 minutes I instruct them to stop wearing the appliance and call to come in for an appointment. A very small percentage of patients may find it difficult to find intercuspal position once their muscles are deprogrammed. This is the appliance doing exactly what we expect it to, and requires patient ownership of the outcome. An important patient instruction is that the appliance not be worn more than 6-8 hours out of every 24. Patients need to understand the risk of tooth movement, although slight, if they wear the appliance more hours than recommended.
After fabrication of a QuickSplint®, plan a follow-up appointment with the patient. First on the list is to find out how they are feeling and what they have experienced while wearing the device. I never cease to be amazed at how many of my patients answer this first question by taking out the QuickSplint® and showing me the wear patterns on its surface and asking “What do we do about this?” Repeat muscle palpation can help both patient and dentist to assess the effectiveness of the QuickSplint® along with new range of motion measurements.
The next step in comprehensive patient care is to fabricate a permanent appliance in the patient with parafunction and for the restorative patient, is gathering centric relation bites for a diagnostic workup. In some patients, the next step is discontinuation of use for an acute pain problem such as an endodontically hot tooth for a brief period of time, or a sprain strain patient.


QuickSplint tray filled with VPS

Patient Bites down to level occlusal table
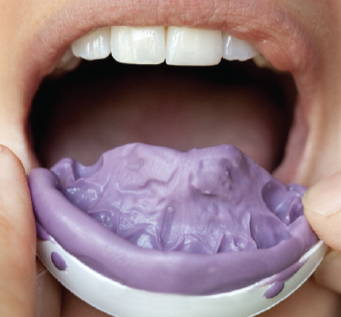
VPS is set, ready for trimming

Grind marks are often evident
Transitional Treatment is the Ultimate Case Acceptance Tool
A gift of incorporating a simple transitional appliance as a diagnostic and therapeutic service is the multiple appointments that let you get to know the patient and build a relationship. In some cases, initial therapy with QuickSplint® results in a final treatment plan with a custom full arch appliance. If the patient feels better, and they are happy with this as an end result, the functional risks are minimized and I have no complaints. For other patients, QuickSplint® is the beginning of a more comprehensive restoration of the health, beauty and function of their teeth, joints and muscles.
Parafunction is one of the greatest problems affecting the dental patient. It is being associated with tooth and material destruction as well as airway risk. Active identification and prompt treatment for this condition is quickly becoming a standard of care. QuickSplint® is your solution to this diagnostic group of patients.
The essence of any anterior only appliance is that is discludes the posterior teeth in all mandibular positions, limiting the contact to the anterior teeth. This design has a predictable effect on the elevator and positional muscles, joint loading and therefore the patient’s signs and symptoms. The design is highly efficient: as the muscles release and the joint position changes, the lack of posterior contact eliminates the need for follow-up adjustments to eliminate posterior interferences that are dependent on condylar seating.
The elevator and positional muscles fire in response to the contact of the teeth. When posterior teeth are in contact it increases the activity of Masseter, Medial Pterygoid and Temporalis muscles. This effect occurs in both intercuspal position and excursive movements. The Lateral Pterygoid muscle fires to brace against the elevator muscles when they fire. Additionally the Lateral Pterygoid fires to position the condyle and allow the patient to smoothly close into their intercuspal position. The first point of contact in centric relation directs this coordination of muscle firing, known as an engram. When we eliminate a first point of contact on a posterior tooth, the Lateral Pterygoid will release and allow the condyles to seat. Joint loading is a function of muscle activity, tooth contacts and condylar position. Because of the interaction of these three factors we can‘t follow a linear thought process to predict the impact of an anterior-only appliance on joint loading, and therefore patient comfort.
About the Author

Lee Ann Brady, DMD
Lee Ann Brady is a internationally recognized educator, lecturer, writer, and is the Executive Director at the Pankey Institute.
Dr. Brady is the founder of RestorativeNation.com, a private social network and dental learning community. She also maintains a private practice in Glendale Arizona.
Discover More
This article was originally published in the Clinical Life™ magazine: Winter 2022 edition
Clinical Life magazine is a premier periodical publication by Clinical Research Dental Supplies & Services Inc. Discover compelling clinical cases from Canadian and US dental professionals, cutting-edge techniques, product insights, and continuing education events.



